How we are paid for behavioral health is evolving quickly. In 2025, providers will have to navigate a lot of new codes, policies, and technologies.
Demand for mental health and substance use treatment grew during the pandemic. Telehealth visits for care grew from around 1% prior to 2020 to more than 32% in the first half of 2022.
This growth is backed by policy developments: Medicare permanently extended home-based telehealth care and audio-only visits, and private payers are broadening coverage. Meanwhile, new rules and CPT codes are in the pipeline. As a result, billing specialists and physicians must keep up with reimbursement rules on telehealth, digital therapies, and coordinated care.
The good news is that these developments also enable new ways to make money and deliver care. Below, we outline the top behavioral health billing trends of 2025, contrast them with the 2020 to 2023 timeframe, and provide helpful advice for physicians in this space.
Telehealth Expansion Continues for Behavioral Health Billing
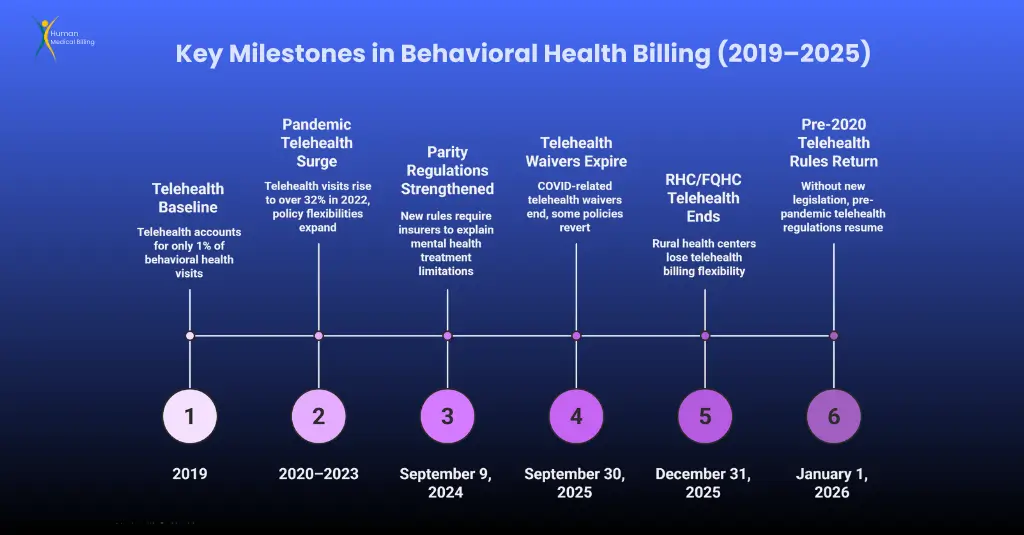
Telehealth has transformed behavioral health care. Its use surged during the pandemic and has stayed high ever since. Telehealth represented about one third of all behavioral health visits by 2022, up from only 1% in 2019.
Medicare now covers almost all behavioral health care through telehealth, enabling patients to access care from home and utilize audio-only visits. In fact, the HHS telehealth policy page indicates that “Medicare patients can permanently receive telehealth services for behavioral/mental health care in their home”.
Commercial payers and Medicaid plans have followed suit, usually by expanding telehealth options or copying Medicare. For instance, new bipartisan legislation (the Telehealth Modernization Act) is set to allow home-based telemental health on a permanent basis and end the need for an in person visit every 6 months.
These telehealth expansions have two significant effects on behavioral health billing. First, providers can see more patients (rural and homebound) and bill at the same rates as office visits. Medicare now reimburses for tele therapy (CPT 90834-90838) and psychiatry services under the same rules as in person care, minus the former geographic restrictions.
Second, documentation rules still apply: physicians need to use the correct telehealth codes (e.g., “95” or “GT”) and document where and if consent was received.
Clinics must review each payer’s most recent policies some will terminate the COVID related waiver after September 30, 2025. (For instance, general telehealth waivers expire then). In short, telehealth will still be crucial to behavioral health billing in 2025, with expanded access and dollars, but it requires strict adherence to evolving rules.
Digital Therapeutics and Remote Care in Behavioral Health Billing
Digital health is another fast growing piece of behavioral health billing. In 2025, Medicare will begin covering certain digital mental health devices and apps.
The CMS 2025 Physician Fee Schedule final rule establishes new HCPCS codes (e.g. G0553 G0554) to reimburse FDA cleared “digital mental health treatment devices” used under a clinician’s plan of care.
These codes allow providers to bill for the use of prescription digital therapeutics (such as CBT apps or digital ADHD treatments) alongside traditional therapy.
Although only a handful of devices meet CMS criteria now, this is a groundbreaking move a recent report called Medicare’s proposal “a breakthrough for health tech”.
In practice, doctors will need to document that the patient uses the specific digital device, and bill the new HCPCS code in addition to any standard therapy code.
Beyond digital therapeutics, other remote monitoring tools are increasingly billable. For example, the 2022 CPT update introduced remote therapeutic monitoring (RTM) codes (98980 98981) which cover services like tracking a patient’s mental health or cognitive therapy data remotely.
While these codes are mainly used by therapists, physicians involved in remote care coordination should be aware of them. Similarly, remote patient monitoring (RPM) CPT codes (99453 99457) can apply if patients use monitoring devices (even for mental health parameters).
Providers should assess whether their practice can leverage RPM/RTM billing (for example, monitoring a patient’s anxiety or sleep patterns via apps) to boost revenue and engagement.
The net effect is clear: digital care opens new revenue streams. Psychiatry and counseling practices can, for the first time, generate reimbursement by prescribing and supporting digital tools.
This will involve integration with IT systems (to monitor device usage and patient reported information) and diligent coding. But combining old school therapy with technology has potential it’s a trend built on the 2020 to 2023 telehealth explosion, when convenience and innovation became the focus of patient care.
Medicare and Regulatory Updates Impacting Behavioral Health Billing
Some 2025 Medicare rule revisions actually affect behavioral health billing directly. Most notably, perhaps, the CY2025 Physician Fee Schedule (PFS) final rule institutes a modest pay reduction:
Medicare’s conversion factor drops ~2.93%. (From $33.29 to $32.35), reflecting the end of a temporary 2024 bonus. This means average payments for services like psychiatric visits are 2 to 3% less than in 2024.
Congress is weighing reducing this cut (the proposed Medicare Patient Access and Practice Stabilization Act would move the cut from –2.8% to a +1.9% increase), but doctors can anticipate tighter profit margins.
But CMS is addressing several measures to enhance behavioral health access. A few notable final rule provisions are:
Safety planning interventions:
CMS has finalized a new G code (G0560) for suicide prevention safety planning by a qualified professional. It can be billed in 20-minute units when the professional develops a safety plan face to face with an agitated patient.
There is also a bundled follow up code (G0544) for up to four monthly phone checks following a psychiatric hospitalization or emergency room visit. These codes appreciate the valuable aftercare work of psychiatrists and counselors and have specific documentation requirements (e.g., detailing the safety plan or phone discussion).
Digital mental health devices:
Three new HCPCS codes for FDA approved digital treatments. To bill for them, you must demonstrate a patient’s use of an approved device or app as part of a treatment plan. (CMS will monitor use patterns to inform future policy.).
Interprofessional (consultation) codes:
CMS added six new G codes (G0546 G0551) to pay mental health professionals to talk with other clinicians about a patient’s care. They are analogous to physician E/M consult codes but are for psychologists, social workers, counselors, and others who are not paid for casual consultations.
For example, a 30 to 60 minute case discussion by a clinical social worker can use one of these new codes.
Opioid treatment flexibilities:
It finally pays non MD mental health professionals when they work with peers. Opioid treatment changes: The permanent rule permits some telehealth applications in Opioid Treatment Programs (OTPs) permanently.
OTPs are now permitted to perform initial assessments using audio only telehealth and bill for an intake service (HCPCS G2076) when initiating methadone treatment. CMS will also increase payments for screening social determinants of health (SDOH) in OTPs, acknowledging the additional work of comprehensive addiction care.
OTPs should take note of these rule changes and bill with the new remote counselling and intake add ons billing codes where appropriate.
Telehealth policies:
CMS has extended nearly all Medicare telehealth waivers through 2025. In person requirements for telemental health are waived through at least Sept. 30, 2025, and RHCs/FQHCs can still bill for distant telehealth visits through Dec. 31, 2025.
But, without a new law, all non MH telehealth regulations of the 1990s will return on Jan. 1, 2026. (Lawmakers are discussing extending these flexibilities further.).
Practices should note these end dates in case Congress or CMS makes further changes.
Medicare, Medicaid, and private insurers all are coming together to cover mental illness on the same level as other forms of health care.
In 2024, new regulations were strengthened: on September 9, 2024, regulations were put into place requiring health plans to review and explain any treatment limitation disparity between mental health and medical treatment.
This requires insurers to make prior authorization, network availability, and behavioural health care management no more restrictive than medical or surgical care. Simply, 2025 will see greater scrutiny of why insurers are rejecting claims
They will be required to gather information and take action if more restrictive policies create significant disparities in access to care.
Physicians should be familiar with these regulations and expect insurers to request detailed paperwork to demonstrate that treatment is necessary and complies with any plan regulation.
CPT Coding and Documentation Updates for Behavioral Health Billing
Staying on top of coding changes is critical. Time based psychotherapy codes remain the foundation of BH billing: CPT 90832 90838 for psychotherapy, and 99202 99215 for E/M visits with psychiatric diagnosis. But new codes have been introduced.
Key 2025 billing codes include:
- G0560 (Safety planning): As above, billable in 20 minute increments when a clinician develops a suicide prevention plan for a. Document the intervention details, rationale, and patient comprehension.
- G0544 (Post discharge follow up): covers four monthly phone check ins after a crisis. Patient consent (verbal or digital) may be obtained upfront or during the first call, as allowed by CMS.
- G0553/G0554 (Digital therapeutics): newly established for Medicare payment of approved digital mental health. These are HCPCS codes (not CPT) and should be used only when the patient’s treatment plan includes a cleared digital device that the clinician is managing. Practices must have documentation that the patient accessed the device and how it integrates into care.
- G0546 G0551 (Interprofessional consults): for virtual or phone consults between a behavioural health specialist and another. For example, if a licensed counsellor spends 15 to 20 minutes discussing a case with a psychiatrist via EHR messaging or a quick call, they may bill G0546/G0547 depending on time. These codes require written beneficiary consent and documentation of the consult content and outcome.
- Behavioural health integration (BHI) codes: While introduced earlier (2017 to 2021), CoCM codes (99492 99494 and G2214) and general BHI (99484) remain important. In CMS guidance, these are defined as care management services with a psychiatric. For instance, a PCP billing CoCM must track a behavioral health care manager’s minute. These codes have been available for years, but increasingly primary care practices and psychiatrists use them to bill collaborative care. Providers new to integrated care should review the 2024 MLN booklet on BHI.
- OUD/Buprenorphine codes: OTP services have many codes (see CMS OTP guidelines). For example, HCPCS G2076 covers the initial telehealth evaluation for methadone intake. There are also “bundled medication delivery” codes G2067 G2073 for weekly episodes of care, and add ons like G2079 for take home buprenorphine supply. Additionally, CMS introduced new codes for extra counselling time (G2080), naloxone distribution (G2215/G2216), and peer support (G0536). Provider’s billing OTP should review the latest CMS OTP fee schedule (published annually) to ensure correct use of the over a dozen related codes.
Physicians must also watch document requirements. Insurers are tightening scrutiny of behavioral health claims.
For every code above, thorough notes are essential: include diagnosis, medical necessity, intervention details, and time spent.
For telehealth services, document the modality (video or phone), patient consent, and any limitations (e.g. connectivity issues). Where codes have strict units (like G0560 safety planning in 20 min units), use timestamps or timed entries in the chart. If a state Medicaid or commercial plan has additional requirements (for example, some require specific psychosocial assessment forms before approving therapy), incorporate those into intake processes.
In short, precise documentation is the linchpin of successful behavioral health billing in 2025. Practices should audit a few recent claims with new codes to ensure charts meet all criteria.
Finally, remember ICD 10 CM changes. While not new CPT codes, the 2024 updates added or revised some mental health and SUD diagnosis codes. For example, new codes for cannabis use disorders, neonatal abstinence (maternal opioid exposure), and unspecified neuropsychiatric disorders exist. (The APA’s DSM 5 TR update lists 2024 code changes. Make sure your coding team uses the latest ICD 10 CM manual or software updates so that diagnoses billed match current code sets.
Challenges and Opportunities in Behavioral Health Billing
Even as behavioral health billing opportunities grow, challenges remain. Many behavioral health practices still struggle with insurance denials and delays. Common hurdles include:
- Prior authorizations. Despite parity rules, mental health services often require PA. For example, longer therapy courses or specialty care (psychiatric residential treatment, inpatient therapy) still need payer sign off.
New administrative mandates (like documenting all comparative analyses of NQTLs may help, but until enforcement catches up, expect continued PA headaches. Proactively, verify benefits before appointments and submit detailed necessity letters when required.
- Complex benefit design. Commercial plans and Medicaid vary widely. Some Medicaid programs reduced telehealth coverage post 2020, others maintain it. Psychology vs. psychiatry coverage can differ (some plans limit LCSW visits). Medication assisted therapy (MAT) coverage can also be uneven.
Practices should routinely check patient benefits and even consider hiring a specialist or using software to track payer rules.
- Low reimbursement rates. Behavioral health often pays less than comparable medical services. The Medicare pay cut (–2.93%) compounds this pressure. Commercial plans sometimes reimburse BH at lower percentages of charge.
To counteract, clinics may need to adjust fee schedules or seek alternative revenue streams (like the digital codes mentioned above). Group practices might use this time to negotiate better rates, citing parity and the shortage of MH providers.
- Documentation burden. Payers are demanding more detailed notes. For example, digital therapeutics coding requires proof of device usage, and OTP codes require logs of medication dispensing.
Physicians already strapped for time may find charting more onerous. An opportunity here is to invest in scribes or billing workflows that prompt for required elements. Proper documentation not only secures payment, it also improves patient care continuity.
On the opportunity side, behavioral health demand continues to climb. The behavioral health market has grown in revenue share and in telehealth penetration.
For providers, this means a larger patient base. The expanded telehealth permission lets practices serve patients across state lines (subject to licensing), potentially reaching underserved areas.
New parity enforcement and provider reimbursement codes signal that policymakers are recognizing the value of mental health care. Additionally, integrated care models (like CoCM) are being actively promoted by payers and health systems, which means primary care settings will increasingly seek BH partners. Practitioners who align with these models can access shared savings or coordination fees.
In substance abuse treatment specifically, 2025 brings gains. The ability for OTPs to provide at home telehealth and bill for extra counseling time will improve retention and funding for SUD programs.
Medicare now fully covers methadone and buprenorphine MAT (via the OTP benefit), reducing financial barriers for patients. Clinics should proactively bill newly eligible services (e.g., SDOH screening in OTPs and educate staff on these codes. Integrated care also offers opportunity.
Many insurers encourage screening for depression/anxiety in primary care, and will reimburse for the brief intervention (CPT 99408/99409 for SBIRT are a bit older codes, but still relevant). Collaborative Care (CoCM) is an evidence based model often reimbursed at higher total rates than standalone visits, and it allows psychiatrists to be consultants billing specialized codes.
By partnering with primary care practices, psychiatrists can bill these care management codes, increasing both revenue and patient reach.
In summary, 2025’s mix of challenges (denials, payment cuts, complex regs) and opportunities (higher demand, telehealth access, new codes) makes it imperative for practices to be proactive. The evolution from 2020 to 2023 telehealth emergency use to now a stabilized, nuanced system shows that adaptive providers can grow.
Looking Back: 2020–2023 Trends in Behavioral Health Billing
To appreciate 2025, it helps to recall recent history. 2020 to 2021 were dominated by the COVID 19 telehealth explosion. Emergency waivers allowed almost any provider to see Medicare patients via video (and phone) from anywhere.
Behavioral health visits skyrocketed as shown above. Insurers generally relaxed rules, and providers learned new workflows overnight.
2022 to 2023 saw many temporary rules extended and some permanent changes. The Consolidated Appropriations Act of 2021 had already expanded telehealth by allowing patients at home through 2023. In 2022, Medicare recognized digital health (by proposing and then finalizing the RTM codes) and introduced new mobile health applications coverage.
Telehealth use remained high post pandemic, especially for psychiatry. Meanwhile, policymakers began tightening parity enforcement: in Sept. 2024, federal MHPAEA regulations were updated for the first time in years, and an APA proposed rule was released in 2023 to close loopholes.
By contrast, 2025 is a year of transition. We still benefit from pandemic born flexibilities, but some are sunsetting. Medicare’s 1990s telehealth restrictions will return after 2025 unless Congress acts (for example, requiring in person visits after 2025 will come back unless repealed). On the other hand, 2025 cements many of the beneficial changes: permanent tele behavioral care, new reimbursement codes, and legal momentum on parity.
Compared to 2020 to 2023, physicians in 2025 will experience more stability (many changes are now codified) but also more complexity (multiple new codes and requirements to manage).
Things Clinicians Can Do for Effective Behavioral Health Billing
To manage this complexity, here are some useful things to know:
- Stay up to date. Read CMS updates regularly (e.g., PFS final rules and MLN articles) and professional organization digests. Websites like CMS.gov or specialty societies (e.g., APA, NBCC) provide fact sheets and webinars on billing updates. You may wish to subscribe to Medicaid bulletins for your state.
- Or, for a one-stop source that consolidates key updates and insights, check out this trusted resource with the option to subscribe to a weekly newsletter.
- Train Your Staff. Ensure your clinical and billing staffs are educated on the new codes. Hold a meeting on the 2025 HCPCS/G code updates. Modify your EHR templates to enable safety planning, OTP counseling, and electronic therapy information to be easily documented.
- Confirm Insurance Benefits Ahead of Time. Telehealth and digital health benefits can be different for each insurance company. Train front desk staff on whether the patient’s plan covers tele therapy, what codes to use, and whether prior authorization is needed.
- For new offerings like digital therapeutics, make sure to confirm whether the patient needs a prescription or special authorization.
- Document everything. For every mental health claim, the notes must state that medical treatment is needed. Because of the increased focus on equality, document as much clinical data as you would document for a medical visit.
- Document treatment plans, objectives, risk evaluations, and outcomes. For example, if you are billing for distant device use, explain how the data is tracked and used in treatment.
- Maximize Telehealth Workflow. Telehealth is not disappearing anytime soon, so make your workflow more efficient: keep a good quality video/phone line, acquire telehealth consents in written form, and use HIPAA compliant platforms.
- Document the mode of service delivery in your note clearly (e.g. “Verbal consent obtained for telehealth session via Zoom”). This prevents payment issues.
- Take Advantage of New Codes. Don’t let the new codes for billing pass you by. Use checklists so that when a patient is prescribed a safety plan, the code G0560 is utilized.
- When a patient starts a digital therapy, ensure that your office can track its usage and bill the digital device code. Small coding modifications can create significant revenues.
- Work with Integrated Care. As a therapist or psychiatrist, think about working with primary care. Using special billing codes (G0546 G0551) or joining CoCM can bring in new patients and business. For pediatricians or internists, think about using BH codes like 99484 or CoCM if you have BH staff.
- Advocate and Prepare for Parity. Educate your administrative staff regarding the new regulations of MHPAEA. Gather statistics on any payer denials that look suspicious (e.g., if psychotherapy visits are denied more frequently than similar medical visits). Monitor any request for parity analyses; having records may save your practice.
- Check Technology Investments. Consider the use of practice management software or clearinghouses that alert for new codes. For instance, some billing systems will prompt G0560 automatically when a crisis note is created. Telepsychiatry systems that have the ability to bill can minimize missed claims levels.
- Track Denial Trends. Keep a close eye on your denial and appeal rates. If you have many claims denied for lack of information or coding mistakes, update your intake and documentation questionnaires.
Or, if you notice that a payer is paying well for something (like OTP counseling), take advantage of it by producing more of the service (if appropriate for the patient). By doing so, physicians and clinics can make the 2025 behavioral health billing environment work in their favor.
The behavioral health billing environment is evolving in 2025, and it’s both opportunity and challenge. he following three trends are observable:
telehealth is now permanent for behavioral/mental health care, new virtual codes are coming, And you can expect continued pressure for stricter parity enforcement from insurers, aiming for equitable coverage.
For your practice, Q3 2025 demands informed adaptation. Staying ahead ensures financial stability and uninterrupted, high-quality patient care.
