Medical credentialing is the pivotal process of checking the credentials, licenses, and background of healthcare providers. In 2025, it will see radical transformations.
As healthcare continues to transform further, Medical Credentialing in 2025 will need greater attention, velocity, and active monitoring than ever before.
The new regulations this year require healthcare organizations to keep up with diminishing verification time, ongoing monitoring requirements, and greater focus on data transparency and equity.
This article describes what these changes are, how they affect Credentialing Verification Organizations (CVOs), and what your organization must do to meet NCQA standards and federal regulations.
NCQA 2025 Standards: What's New
The National Committee for Quality Assurance (NCQA) has done significant revisions to its credentialing standards, effective July 1, 2025.
They were completed in August 2024 after public feedback, and they ensure credentialing processes keep up with today’s technology and regulations.
NCQA President, said that these amendments were enacted in an attempt to “align standards to the changing market environment, stakeholders’ needs, and regulatory mandates.”
The guidelines have two important enhancements: timelines for credentialing have been shortened, and ongoing monitoring is now a required element.
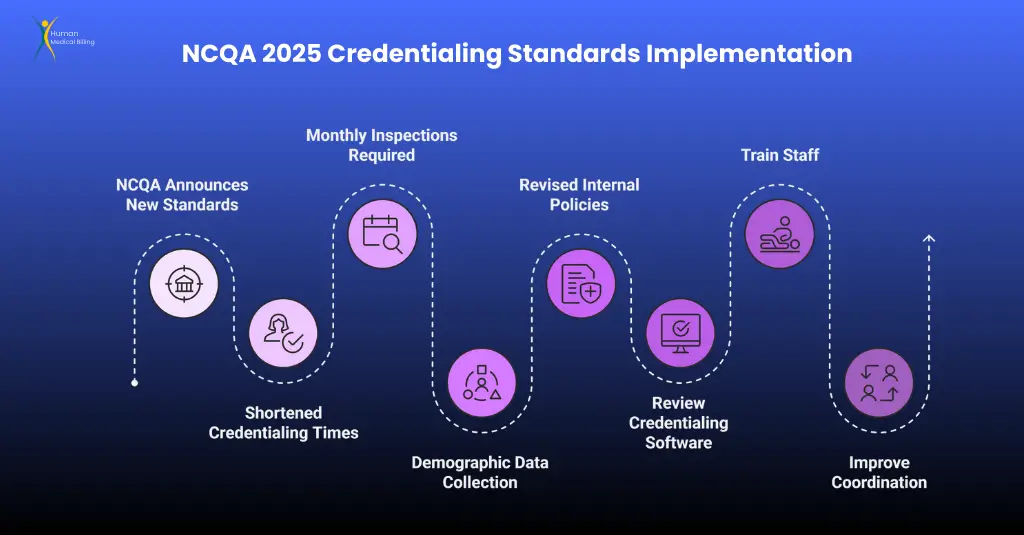
1. Shortened Credentialing Times
Organizations that have been certified by NCQA will now have to follow quicker verification guidelines. Therefore, providers must be credentialed nearer to decision times, enhancing freshness of data and minimizing risks.
- For NCQA-Accredited Organizations: The verification time for primary sources has been reduced from 180 days to 120 days.
- For NCQA-Certified CVOs: The timeline is extended from 120 days to 90 days.
Initially, NCQA proposed the use of universal 90 days but revised later after industry comments. These time frames are made to ensure the provider information remains up to date, particularly licensing and sanctions.
Your organization is required to complete credentialing by July 2025 in 4 months to be accredited and 3 months to be CVO certified.
These changes show a bigger trend: Medical Credentialing in 2025 will focus on being accurate right away and processing quickly.
2. Monthly Inspections Are Required
Before, checking provider credentials was done every 6 months or only upon recredentialed status (usually every 2–3 years). That is no longer acceptable under NCQA’s 2025 regulations.
Organizations will now have to review every provider every 30 days for any problem. This new monthly requirement applies to any credentialing file that was processed on or after July 1, 2025.
Major monthly surveillance tests now encompass:
- License Status and Expiration: Monitor all licenses to anticipate expirations ahead of time. Lost lapses can now jeopardize compliance in a serious manner.
- Medicare/Medicaid Exclusions (OIG): Screen the HHS Office of Inspector General’s LEIE database monthly. Any provider listed here cannot enroll in federal programs.
- Disciplinary Actions and Sanctions: Monitor state medical boards and licensing agencies for any new disciplinary actions, and respond in a timely fashion.
- SAM.gov Verification: Effective 2025, organizations shall be mandated to verify SAM.gov. This is a website displaying individuals and entities excluded from transacting business with the federal government.
Monitoring needs to be documented and reported to the credentialing committee or the peer-review group assigned when problems occur. In short, Medical Credentialing in 2025 is a forward-looking process, not a backward one.
3. Prioritize Fair Data and People Groups
In addition to more stringent controls and verifications, NCQA now mandates demographic information to be collected during credentialing. Applications must include optional fields for:
- Color
- Background
- Spoken languages
Providers are not required to enter this information, although NCQA advises collecting this data to better serve health equity.
This allows health care organizations to be informed regarding the diversity within their network of providers and to have options available for care matching language or culture.
This policy promotes overarching industry goals to mend gaps in healthcare provision and enhance outcomes for poorly served populations.
4. Primary Effects for Your Company
Here’s what your credentialing team must do to prepare:
- Revised Internal Policies: Have your procedures incorporated the new 120/90-day verification requirements and monthly monitoring.
- Review Credentialing Software: Your system should help you collect credentials in an efficient manner and automatically check license status, OIG exclusions, and SAM.gov flags on a 30-day cycle.
- Train Staff: Train the credentialing and compliance staff on these new standards and how to implement them by July 1, 2025.
- Improve Cross-Functional Coordination: Monitoring is no longer a one-time, single-dimensional process. Teams need to coordinate in close proximity to ensure nothing gets in the way.
Satisfying these needs may be achieved by bringing in more personnel or by putting money into equipment to enable monitoring and checking.
5. A Future Perspective
These changes redefine healthcare credentialing compliance.
The movement toward decreasing windows of verification and proactive monthly monitoring is a sea change in regulatory expectations.
If you’re still on a biennial or triennial recredentialing cycle without monthly tracking, you’re already behind.
Medical Credentialing 2025 is all about being accurate, fast, and responsible.
Organizations that transition early will stay in compliance with regulations and minimize risks while having improved patient safety.
In short, the future of Medical Credentialing has arrived – and it’s faster, stronger, and smarter.
Credentialing in the Spotlight:
With the evolving healthcare environment, Medical Credentialing in 2025 is still crucial in establishing trust with physicians and providers and safeguarding patients.
In essence, medical credentialing verifies healthcare providers are qualified and authorized to treat patients.
Conducted in-house or outsourced to third-party vendors, credentialing must adhere to strict standards by organizations such as NCQA, CMS, and OIG.
Credentialing Fundamentals: What is PSV and What are CVOs?
Understanding the language of credentials is essential to ensuring an compliant process.
Primary-Source Verification (PSV)
PSV is the best way to authenticate medical credentials in 2025. It describes authenticating a healthcare professional’s credentials – like their education, licenses, and certifications – directly with the source or an authoritative source.
For example, a medical license is authenticated with the state medical board, and board certification is authenticated by the American Board of Medical Specialties (ABMS).
CAQH defines PSV as “the process whereby a health plan or hospital verifies an individual provider’s self-reported credentials and qualifications.”
PSV is essential; organizations like NCQA and The Joint Commission require that credentialing is performed on the basis of formal verification – not photocopies or self-reporting.
Typical primary sources include:
- Medical school transcripts
- Residency/fellowship certificates
- State licensing boards
- DEA registration (to allow prescribing)
- Specialty certification boards
PSV guards against counterfeit credentials and ensures that only competent individuals can offer care.
2. Credentialing Verification Organizations (CVOs)
A CVO is an organization that performs PSV for healthcare organizations. NCQA defines a CVO as an organization that verifies credentials from primary sources but does not issue final credentialing determinations.
CVOs perform the legwork of calling schools, boards, and registries to confirm credentials. That is why hospitals and health plans like to hire them.
NCQA-certified CVOs are hired by many organizations to perform this work because their processes are held to national standards.
Benefits of using a CVO include:
- Faster provider onboarding
- Decreased administrative burden
- Improved follow-up with verification schedules
- Enhanced consistency and scalability
Even if you use the services of a CVO, your credentialing committee has to make the ultimate decision to approve.
CVOs verify, not credentialing authority. Organizations that are going through Medical Credentialing in 2025 tend to outsource such complicated processes to experts.
For example, Human Medical Billing offers comprehensive credentialing services that are NCQA and CMS compliant.
Services are offered including PSV, license tracking, and monthly exclusion reports.
In short, PSV is the key element of credentialing, whether organizational or through a CVO.
Federal Oversight: CMS, OIG, and SAM.gov Expectations
In 2025, credentialing is impacted by NCQA and federal agencies. Compliance with the regulations is mandatory in order not to incur fines, overpayments, and loss of the capacity to accept Medicare or Medicaid.
1. OIG Exclusion Monitoring
The LEIE (List of Excluded Individuals/Entities) is preserved by the United States Department of Health and Human Services Office of Inspector General (OIG).
Excluded providers are ineligible to take part in federal healthcare programs such as Medicare or Medicaid.
There is no law that mandates how often providers must query the LEIE, although the OIG strongly advises they do so at least once each month.
Within its Special Advisory Bulletin, the OIG stated that monthly checking of employees and contractors “best minimizes potential overpayment and CMP (civil monetary penalty) liability.”
Since 2011, CMS regulations (42 C.F.R. § 455.436) have required state Medicaid agencies to verify the LEIE each month. Due to this, nearly all health plans and provider organizations now perform monthly OIG screening in order to prevent compliance issues.
If the provider appears on the LEIE, he or she must be removed from billing or practice immediately to prevent federal penalties.
2. SAM.gov verification
SAM.gov (System for Award Management) is the repository of the government-wide exclusion database, once known as the GSA’s Excluded Parties List System (EPLS).
Although LEIE is healthcare-specific, SAM.gov maintains federal debarments from all of the agencies, including those providers excluded from federal contract awards for fraud or misconduct.
In 2025, NCQA added SAM.gov to its monthly required check, in addition to the OIG list. While OIG LEIE provides more health-care-related information, screening both is now best practice to best ensure effective exclusion screening.
The majority of credentialing systems now package these screenings, rendering providers compliant with both federal databases.
3. CMS and Credentialing Regulations
The Centers for Medicare & Medicaid Services (CMS) have a direct impact on credentialing through the following:
- Medicare Advantage Plans: These plans must credential and recredential providers every three years as mandated by CMS. The majority of Medicare Advantage organizations utilize NCQA accreditation to meet this mandate.
- Hospitals: Hospitals are required under CMS Conditions of Participation to verify credentials via PSV and reappoint physicians biennially. The ultimate determination should be made by a governing body or medical staff committee.
- Telehealth: CMS has recently updated regulations to permit credentialing by proxy to enable hospitals to credential telemedicine providers via partner facilities. CMS in 2025 is also addressing state licensure of telehealth to ensure providers are licensed in the state in which care is being received.
In effect, CMS follows NCQA standards and requires credentialing processes to be done quickly, thoroughly, and well-documented.
4. Don't Miss State-Level Regulations
This article refers to national and federal accrediting bodies, yet we must remember state-based requirements as well. The majority of states:
- Require non-discriminatory credentialing decisions
- Require timely application processing
- Use central databases like CAQH ProView.
- Implement CMS/OIG monthly exclusion screening guidelines.
Before you finalize your credentialing policy, make sure your organization takes into account state laws as well as federal regulations.
In Brief: What Medical Credentialing in 2025 Requires
In 2025, as Medical Credentialing transforms, healthcare organizations need to ensure that their processes meet both accreditation and regulatory standards.
Credentialing is no longer a static, one-time process; it is now an ongoing, active process.
To remain compliant and protect patients, organizations should:
- Verify all credentials through primary sources
- Employ qualified CVOs where required to increase efficiency
- Check the OIG’s LEIE and SAM.gov on a monthly basis.
- Follow CMS and NCQA regulations for recredentialing cycles (every 2–3 years)
- Ensure telehealth providers are appropriately licensed
- Stay informed about and compliant with state regulations
Failure to observe these practices can result in fines and patient harm, as well as reputational harm. Credentialing is an effective risk management strategy, from fraud protection to network security.
Missing a sanction, not capturing an expired license, or having an unauthorized individual on staff can be costly. But with proper systems, partnerships, and vigilant monitoring, your business can stay current with Medical Credentialing in 2025.
Automation in the Workplace: Staying Current with Medical Credentialing Needs in 2025
The Medical Credentialing standards of 2025 are tighter than ever. With quicker credentialing cycles and monthly required checks, medical groups can no longer depend on outdated manual processes and stale spreadsheets.
NCQA’s new rules – effective July 1, 2025 – have spoken clearly: credentialing needs to be quicker, more precise, and checked regularly.
In order to be able to comply with these stringent regulations, automation is no longer an option but a requirement.
In fact, NCQA has stated that its 2025 standards require organizations to use technology in order to be compliant.
In this article, we describe how automation ensures compliance, reduces risk, and has you audit-ready at all times in the new regulation for Medical Credentialing in 2025.
Why Automation Is Important Now
Those days have passed when credentialing teams manually used to confirm licenses, check sanctions, and track expirations. Today, with verification on a monthly basis, auditing in real-time, and better reporting, credentialing work is too complicated to be done just manually.
This is how automation is transforming credentialing compliance:
1. Auto License Verifications
NCQA’s shortened time to validate licenses (from 180 days to 120 days for accredited organizations) requires accuracy and efficiency. Credentialing software now plays a central role in automating this task.
Modern platforms can:
- Automatically scan state licensing boards for status
- Get supporting documents right away
- Timestamp each verification, verifier name, source URL, and date
These systems do have detailed audit trails, and NCQA now says these are invaluable. They help ensure each credential was validated on time – and provide clear-cut proof in the case of an accreditation survey.
Rather than spending weeks or days on a manual verification, license verification is performed in real-time and documented diligently, according to the Medical Credentialing standards of 2025.
2. Ongoing Sanction Screening
NCQA currently mandates that healthcare organizations check at least monthly all of their providers for sanctions or exclusions.
This would include databases such as:
- OIG’s List of Excluded Individuals/Entities (LEIE)
- SAM.gov (System for Award Management)
- State medical board disciplinary records
Credentialing software may batch screen against these databases on a scheduled basis (e.g., the 1st of each month).
When a provider is identified on a sanction list, the system notifies it for review and notifies the credentialing staff.
Computer-generated reminders are used to ensure that any untoward incident is not left unreported between cycles of credentialing. The system also maintains a history of all the monthly reviews, which is helpful for audit trails and NCQA compliance.
3. Expiration Monitoring and Reminders
A key 2025 improvement by NCQA is that organizations need to monitor when credentials are set to expire. A manual calendar or an Excel sheet is not secure enough.
Credentialing websites now:
- Maintain a current database of all license and certification renewal dates.
- Automated email reminders to providers and administrators
- Send reminders 60 and 30 days prior to expiration.
When a license is about to expire, the provider must shut down operations at once, and this can cause safety and legal issues for patients. Through automation, organizations can prevent missed renewals and show responsibility – two critical elements of Medical Credentialing in 2025.
4. Data Management and Reporting Compliance
With new rules such as demographic data collection and ongoing surveillance, companies need to monitor more data than ever. Reporting is not a back-office activity – it’s a compliance tool.
Credentialing systems offer:
- Compliance snapshots and on-demand dashboards
- Regularly scheduled reports (e.g., providers up for recredentialing next quarter)
- Exportable logs for every verification activity
NCQA prefers organizations to offer verification and monitoring data in audits or surveys. Automation simplifies the process. The files don’t need to be manually pulled. The teams can prepare in-depth reports in a matter of seconds.
Credentialing committees also gain: they are able to view issue summaries and sanction alerts in real-time, which enhances oversight and reduces the likelihood of negligent credentialing.
5. Readiness by Design in Audits
One of the greatest advantages of automation is that you are always prepared for an audit. Whether you have an NCQA site visit, a CMS audit, or a state inspection, having well-organized and easy-to-read credentialing records is extremely important.
Credentialing platforms assure:
- Everything is tracked (who looked at what and when)
- Time-stamped sanction checks are conducted
- Expiration notices are recorded
- Missing gaps, if any, are clearly evident and actionable.
One compliance specialist put it this way: “Keep detailed records of data changes, monitoring gaps, and verification activities – demonstrating a commitment to transparency.”
That’s precisely what new credentialing systems provide. Conversely, manual systems tend to fail under audit, which results in panic, mistakes, or worse – noncompliance findings.
Conclusion: Revitalizing Credentialing for 2025 and Beyond
Medical Credentialing is no longer paperwork – it is a vital safety step that functions each month while a practitioner is practicing. Being precise and vigilant is extremely critical as Medical Credentialing in 2025 becomes busier.
NCQA's new regulations mandate:
- Streamlined verification (120- or 90-day cycles)
- Checking data from various sources monthly
- Demographic data collection for health equity
- Keep records of all checking and reviewing activities.
Federal agencies like CMS and OIG endorse these expectations. Failure to meet them can result in serious issues, such as money fines and patient safety risks.
In preparation, healthcare organizations should:
- Update policies and workflows to match 2025 requirements
- Train credentialing teams in readiness for monthly monitoring and auditing.
- Purchase current credentialing software or hire NCQA-certified CVOs under contract
These steps assist in avoiding compliance problems and facilitating easier addition of new providers, smoother operation of services, and building a more stable reputation.
Ultimately, it’s not so much about technology and regulation – it’s about trust. Trust that each provider a patient encounters has been thoroughly vetted and trained to treat them. That’s what Medical Credentialing in 2025 is all about.
