
Most healthcare providers treat EHR and EMR as the same term, yet they are not the same. That confusion can have very real billing implications. An Electronic Medical Record (EMR) is a digitized version of an individual provider's paper medical record - valuable to that provider within their own clinical setting but unable to be accessed by other providers outside of that environment. An Electronic Health Record (EHR), however, is designed to allow sharing of patient information among multiple providers, facilities, clearinghouses and payers - making it the only system type capable of satisfying all CMS requirements for Medicare reimbursement programs (MIPS reporting & the Promoting Interoperability performance category). For billing teams, the system your practice runs determines whether your claims process cleanly or if they will continue to struggle with avoidable denial of payment.
Quick Answer
- EMRs are used by one doctor or practice only; therefore, they do not allow data sharing across providers or other organizations.
- EHRs are made to support the flow of information across multiple systems and help with checking eligibility in real time as well as clearing house operations.
- Prior to participating in MIPS, CMS has required that all physicians and healthcare providers utilize CEHRT (Certified Electronic Health Record Technology), or else they may be assessed a 9% Medicare Part B payment penalty.
- Physicians who have not transitioned from an EMR system to an EHR system experience greater rate of denied claims, delayed prior authorizations, and lower reimbursement.
The Core Difference Between an EHR and an EMR
Let's take this apart and define these terms so we are all on the same page.
An electronic medical record (EMR) is an electronic version of your chart maintained by your healthcare provider for their records alone. It documents what you have been diagnosed with, what medications you are taking, what tests and lab work were done, and your visits at that office. Your billing department will likely use it to help create documentation for each encounter. The data will be kept in-house. An EMR will not share your information with laboratories outside of their own facility, specialist offices, payors or a health information exchange. Simply put, think of it like a very organized file cabinet that has never left the premises of your provider.
An electronic health record (EHR) provides all of the functionality of an electronic medical record (EMR), with the additional capability to transfer a patient's clinical information electronically through their care continuum. In addition to allowing for the connection to other healthcare providers; clearinghouses; payer systems; and state and/or national health information networks, when a patient visits a specialist physician; has an imaging study performed by another provider; or requires pre-authorization from his/her insurance company, it also allows for the automatic exchange of clinical information required to make these work flows operate smoothly. This exchange of clinical information throughout a patient's care continuum is what sets an EHR apart from an EMR functionally.
The Office of the National Coordinator (ONC) and CMS have consistently used "EHR", as their standard terminology, since EHRs are designed with interoperability in mind - i.e., sharing/receiving health information. EMRs were never designed for this.
What CMS Requires and What Happens When You Don't Meet It
Eligible clinicians and participating hospitals are required to utilize the certified electronic health record technology (CEHRT), as part of participation in the Merit-Based Incentive Payment System (MIPS). The Promoting Interoperability performance category is 25% of an eligible clinician's MIPS total score; thus, it will require that all data be collected from a CEHRT compliant system for at least 180 continuous days in order for it to meet the calendar year requirements.
The above regulation states that a system that will only have Electronic Medical Records (EMRs) does not meet this requirement. A system with only EMRs is NOT CEHRT. Therefore, it can not create the QRDA I files necessary to report electronically on clinical quality measures and it can not meet the objective of exchanging health information. With zero points in the Promoting Interoperability category your total MIPS score will be lowered. If your total MIPS score is below the performance threshold you may experience cuts in payments.
The highest possible MIPS penalty will be 9% for all clinicians whose final scores are at or below 18.75 points. The performance standard remains at 75 points, meaning those clinicians have to hit 75 points to avoid a reduction in their Medicare payments. If a clinician's clinic has annual Medicare part B bills totaling $400,000, an additional 9% penalty would be approximately $36,000 per year. That will continue until the problem is resolved.
The Medicare Promoting Interoperability program is an extension of the HITECH Act that was passed with subsequent updates via MACRA. This program's primary purpose is to require eligible hospitals and clinicians to demonstrate meaningful use of Certified EHR Technology (CEHRT), using CEHRT as the mechanism by which they will provide interoperable health information exchange. Since the requirements have become increasingly stringent. In 2025 all 100% of participants in ACOs are required to utilize CEHRT, whereas previously only a small percentage of participants in these types of programs were required to utilize CEHRT.
How System Type Directly Affects Your Revenue Cycle
Your system will touch on each step in the billing cycle. Here is what that means for your team.
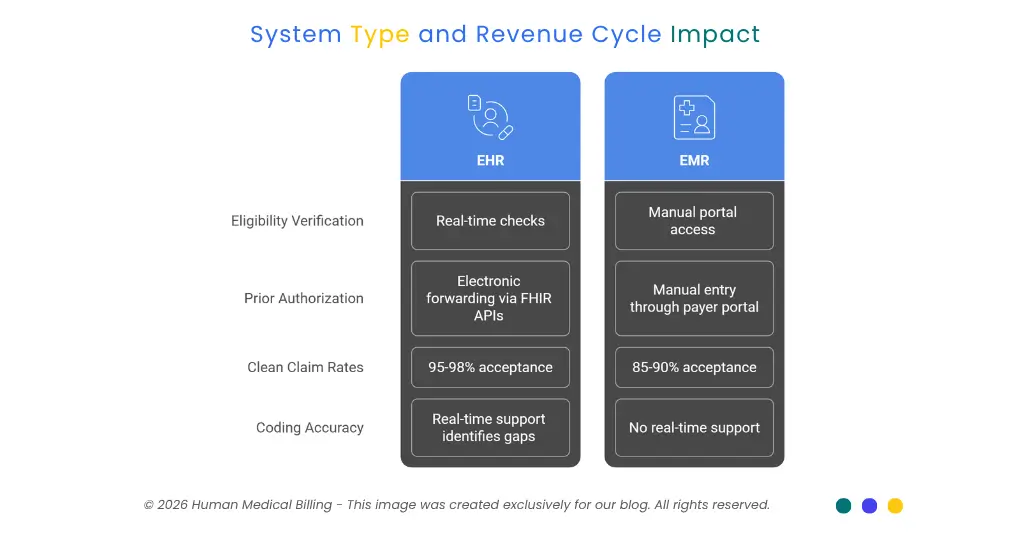
1. Eligibility verification.
EHR's that are integrated into clearing houses allow for real time eligibility checks when a patient presents for care. EMR's do not have the same capability so staff have to access a payers portal to verify eligibility; a less efficient way of doing things that has the potential of more errors early in the claim process.
2. Prior authorization.
The CMS states that processing prior authorization requests costs providers anywhere from $20-$50 per hour, and takes up approximately 13 hours of staff time per week, or roughly $34,000 and 700 hours of employee time annually. Electronic Health Record (EHR) systems that are linked to FHIR based APIs, can electronically forward prior authorization (ePA) requests from the patient's clinical document directly into the system. Staff must enter these ePA requests manually through the respective payers portal when using their Electronic Medical Records (EMR). This adds additional time and increases the likelihood of missed prior authorizations.
3. Clean claim rates.
There is a considerable difference in how often providers have their claims accepted or denied between EHR-integrated billing and standalone billing. Claims acceptance rates for those utilizing EHR-RCM integrated billing are reported as being 95-98%, which is considerably higher than the average rate of 85-90% for non-connected systems. More denied claims equals more denial processing, more time spent on reprocessing denied claims, and extended days in accounts receivable.
4. Coding accuracy.
EHR's with real time coding support will identify missing documentation gaps prior to claims submission. EMR's cannot provide this same capability as it is not designed for interaction with payer-logic. Coding errors that would otherwise be identified in the EHR workflow go undetected in EMR environments, which creates subsequent denial issues that require intervention by denial management services teams.
What This Means for Your Patients and Payers
Patient-centrically, EHRs offer patients an opportunity for portal entry, automatically send appointment reminders, and allow patients to share their medical record with all other providers of care. This is relevant to billing as CMS now links certain quality metrics (patient engagement) to payment in its Promoting Interoperability category. If a practice cannot show that it has a certified system allowing its patients access to their patient- facing health data, then they will be scored lower on those metrics.
For payers, EHRs are the same data language that most insurance companies now need. The CMS has created an electronic prior authorization measure in the MIPS Promoting Interoperability Performance Category; Eligible Clinicians must attest to having submitted at least one prior authorization electronically via a Prior Authorization API, utilizing data from CEHRT, beginning with the 2027 performance year. Therefore, practices without an EHR will be unable to fulfill this requirement when it is implemented.
Policy is moving in a specific direction. The framework for reimbursement (by CMS) will be built with interoperability in mind when it comes to EHR systems. Practices using EMRs alone have two issues - they are both technologically behind and outside of the compliance area that Medicare payment increasingly requires.
What Should Your Practice Do Now?
These are good steps to take now if your practice operates on an EMR or you have concerns about whether your current system meets the definition of CEHRT.
1. Verify your system's certification status.
Look up your ONC Certified Health IT Product List (CHPL) at healthit.gov. If your system is not identified in CHPL as CEHRT compliant then your system is not eligible for meeting the MIPS Promoting Interoperability Requirements.
2. Audit your Promoting Interoperability score.
Review your MIPS performance categories and see if your PI category has automatically had its weight set to zero due to system limitations. That is an indicator that system issues are resulting in lost MIPS dollars.
3. Review your prior authorization workflows.
Determine how many of these authorizations are being processed manually versus tied to your EHR. Manual-only workflows becoming a direct billing liability as the 2027 ePA mandate approaches.
4. Talk to your billing partner
Discuss your current level of system integration with your medical billing services or healthcare revenue cycle management services partner. An experienced RCM team will be able to identify areas in which system failures are resulting in denials, lost incentive opportunities or reimbursement challenges; and assist you in determining priorities based on what needs to be fixed first.
5. Plan your transition timeline.
Transitioning systems takes time. The earlier you begin the planning process to switch from EMR to another EHR, compliant with CEHRT standards; the sooner you will be prepared to meet new CMS mandates versus simply responding to them.
Frequently Asked Questions
The EMR is a digital record of the patient chart utilized by one clinician in one clinic. The EHR is an interoperable, certified platform which allows sharing of patient information among clinicians or providers, payors and healthcare systems. CMS requires the use of EHR based CEHRT for Medicare reimbursement programs.
NO. CMS has made it mandatory to utilize Certified Electronic Health Records Technology (CEHRT) for the Promoting Interoperability performance category; therefore, an electronic medical record is not compliant with CEHRT standards as the ONC certification does not include interoperable functionality. Therefore, if you do use a non-certified system, you will receive no points for that particular MIPS category.
Real time eligibility verifications, automated prior authorizations, and code validations (all through EHRs) are used by clearinghouses and payers for EHRs. With these capabilities, many of the front-end billing issues that lead to claims denials can be identified as you enter the claim into your system. EMRs do not have this capability so when an error occurs in your EMR it is sent to the payer without a resolution.
Failure to use CEHRT for the MIPS Promoting Interoperability performance category will result in zero points for that performance category. This combined with underperforming elsewhere will reduce your overall MIPS score resulting in a possible penalty of 9% of Medicare Part B reimbursement.
Get the Billing Foundation Right
The difference between an EHR (Electronic Health Record) and EMR (Electronic Medical Record), while a non-technical distinction for many healthcare providers is a serious compliance and revenue issue for your practice to consider in 2026. At Human Medical Billing, we work with practices who have technical issues which create reimbursement friction that they do not realize exist. Our medical accounts receivable services and medical coding services were designed to find these issues and fix them. If you want to determine how your current systems affect your revenue cycle, then our team can assist you. Please visit our FAQ's section on our website to see how we can help your practice at whatever stage of billing you may be at.

Contact Human Medical Billing to schedule a compliance readiness review or learn more about our end-to-end billing and regulatory support services.
