The Center for Medicare & Medicaid Services (CMS), after years of extending temporary telehealth provisions related to the Public Health Emergency, has completed establishing a permanent telehealth structure as part of the Calendar Year (CY) 2026 Medicare Physician Fee Schedule (MPFS) Final Rule.
This is NOT another short-term fix; this is the fix.
Beginning with the first day of 2026, "Provisional" telehealth will be nothing but history. The Center for Medicare & Medicaid (CMS) has abolished the "provisional" designation in favor of "permanent", which will fundamentally alter how all practices, billers, and coders consider telehealth.
For medical practices, the permanent removal of frequency limits is a huge operational advantage; however, with that comes new billing and compliance requirements your practice cannot afford to ignore. We will detail the permanent removal of frequency limits, the formalization of virtual direct supervision, and the compliance processes your practice must start immediately.
The End of Telehealth Frequency Limits in Facilities
This is the long-awaited update.
CMS has officially eliminated all frequency restrictions on Telehealth services as of January 1, 2026 for Inpatient Hospitals, Skilled Nursing Facilities (SNF) and Critical Care settings.
Prior to this rule, Medicare had a firm cap on the number of times a provider could submit claims for Subsequent Nursing Facility Care or Inpatient Visits via Telehealth. The cap for SNF's was limited to one per 14 days. This cap arbitrarily restricted the amount of time a provider could provide care, reduce contact with high-risk patients and ultimately pay for the cost of coordinating care which could no longer be billed.
Those days are behind us.
Now, specialists and primary care providers have the ability to treat patients with chronic diseases and post-acute care as long as they wish and regardless of geographical distance or time. This is a real opportunity for those most vulnerable Medicare recipients to receive more regular and consistent care.
"Removing frequency restrictions for telehealth from facility based settings will support CMS's goal of reducing avoidable hospital readmission and enhancing continuity of care for at risk and chronically ill patient populations."
If you bill separately for each of your subsequent inpatient admissions, critical care or skilled nursing facility (SNF) admissions using telehealth, then it is imperative that you instruct your billing staff to begin making the necessary workflow adjustments as soon as possible. Contact your healthcare revenue cycle management service provider so they can verify that your systems will be updated by the time you submit the first claim.
Virtual Direct Supervision Is Now Permanent
This is the second big shift and one with a fair amount of compliance weight behind it.
CMS has permanently allowed supervising clinicians to meet the "immediately available" criterion for direct supervision with either real time (live) two way audio or video technology. Prior to this rule change, all supervisory personnel had to be physically located within the same office suite as the clinician being supervised. Now, it is possible for supervisory personnel to be remotely located using some type of live video technology and meet the Medicare definition of direct supervision.
Here is what that means in practice:
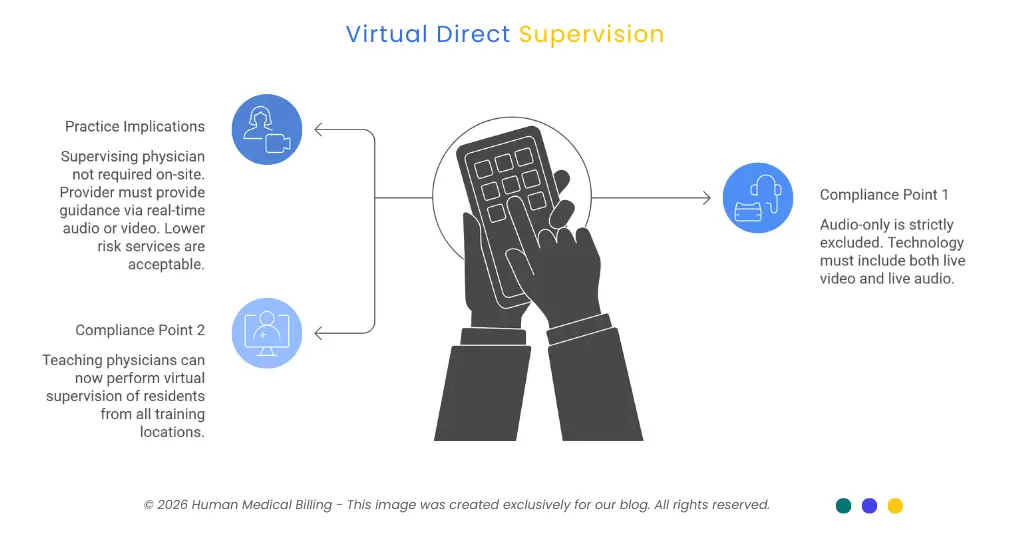
- The supervising physician is not required to be on-site with the auxiliary staff member.
- However, the supervising provider must be able to provide guidance to the auxiliary staff member (via real-time audio or video) at all times that he/she provides an incident-to service.
- Lower risk services, typically those provided as "incident-to", such as services by nurses, medical assistants, etc., are examples of when this is acceptable.
Two compliance points you cannot miss:
Audio-Only Is Strictly Excluded:
The technology used for supervision must include BOTH live video and live audio. Telehealth may be performed via phone call only, but this would NOT meet the criteria for live video/audio and would likely lead to denial of your claim(s) as well as an audit.
Teaching Physicians Are Now Covered More Broadly:
CMS has finalized their rule that teaching physicians can now perform virtual supervision of residents who furnish telehealth services from ALL training locations - not limited to rural locations. This is a significant change for academic medical centers and teaching practices.
In need of assistance in developing your workflow for documenting supervision through telemedicine? The team at Human Medical Billing helps numerous practices each day address similar compliance issues.
2026 Virtual Direct Supervision Rules at a Glance
| Rule Element | Old Policy (Pre-2026 Extensions) | New Permanent Policy (2026) |
|---|---|---|
| Immediate Availability Definition | Supervising physician must be physically present in the office suite | Supervising physician may be present via real-time, two-way audio/video technology |
| Allowed Technology | In-person only for direct supervision standard | Real-time audio AND video required; audio-only is excluded |
| Eligible Services | Limited to services where physician was on-site | Most lower-risk incident-to services furnished by auxiliary personnel; expanded teaching physician coverage at all training sites |
Billing, Documentation, and Audit Risks
Expanded coverage does not mean reduced scrutiny. Let's be clear about that.
Incident to billing and Split/Shared services are still among the top audit targets by the Office of Inspector General (OIG). CMS expanding access does not exempt you from the OIG radar, it could have the opposite effect.
Here is what your billing and coding teams must do right now:
- Document Virtual Supervision Explicitly. Documenting virtual supervision in the EHR must be done explicitly, as physicians have to include documentation about how they were able to provide direct supervision virtually using live video/audio. Simply stating "I was available" is not acceptable and you must state your method.
- Record Time and Involvement. The physician providing virtual supervision has to also document their availability for supervision at the specific time services were rendered and for the duration of those services. This documentation includes timestamp(s). Your electronic health record may have logs of this activity as well.
- Verify Practice Location Enrollment. In addition, if providers are furnishing telemedicine services from their homes, it is essential to verify that all of your practices locations enrolled with Medicare are current and accurate. Misinformation could cause denials or even additional issues.
Your medical coding service team must conduct an audit of your clinical documentation related to incident-to services prior to your next billing cycle. And, if you have already seen increased denials in these areas, it would be best for your denial management services team to alert these specific categories.
If your practice has not been fully credentialed by all payers for all telehealth services, now is the time to address this issue with medical credentialing services.
The Financial Picture: The 2026 Conversion Factor Update
The telehealth news arrives during one of the most positive financial times physicians have experienced in years.
Following on from two consecutive years of reductions in Medicare payments, Congress approved H.R. 1, which includes a short-term 2.5% increase in physician payments. In combination with MACRA, the 2026 MPFS represents an unusual upward payment adjustment.
- Qualifying APM Participants (QPs): Will experience a 3.77% increase in payment, and the conversion factor will be $33.57.
- Non-QP Physicians: Will experience a 3.26% increase in payment, and the conversion factor will be $33.40.
The importance of the above cannot be overstated. A higher conversion factor means every telehealth visit, every incident-to service, every SNF follow-up you appropriately bill is valued higher than it was last year.
Practices that create the correct telehealth billing workflow for 2026 will benefit directly from an enhanced revenue cycle. This is not speculation, this is math. Your medical accounts receivable services team should be calculating these increased rates as part of your expected monthly collections at this time.
To see what an optimized billing process looks like for a practice similar to your own, review our success stories or read through our frequently asked questions (FAQs) to learn how we take a compliance-based approach to billing.
Next Steps: What Your Practice Should Do This Week
The permanent elimination of frequency restrictions and the codification of virtual direct supervision will give providers a clearly defined path to grow their virtual care programs with confidence. Regulatory uncertainty is gone; compliance requirements remain.
Here is your action list:
Train your clinical staff immediately
Immediately train all clinical staff on the required documentation of virtual "immediately available" and have every supervising physician familiarize themselves with the language that should be documented in the EHR.
Audit your incident-to and split/shared billing
Audit your incident-to and split/shared billing on any claims you have already submitted in 2026 so that you can find any documentation deficiencies before an audit is done.
Confirm all practice location enrollments
Confirm that each of your practice locations has been correctly enrolled in the Medicare enrollment data base.
Review your payer contracts
Review your payer agreements to determine where additional telemedicine coverage by commercial payers will be available based upon what CMS is doing first.
As a result of the 2026 MPFS Final Rule, practices that prepare will be rewarded. If you do not have a clean and compliant billing infrastructure in place to collect opportunities created by the new rule, now is the time to correct it.
Want to find out how we assist with the services listed above? Find out how our services function or browse through all of our medical billing service options. Additionally, view the most recent blog posts at the Xpert Billing Blog.
Are you ready to leverage the 2026 rule changes to your benefit? Contact us immediately or get to know us to understand why so many practices from coast to coast rely on Human Medical Billing to safeguard and expand their financial revenues.

